For a drug policy that makes Europe safer, healthier, and more just
Despite billions spent in drug control, European drug policies have failed to protect the health and safety of our communities.
Drug use is reaching historical records. New substances are entering the EU market every year. War-on-drugs policies have been unable to stop the growing power of organised crime. Evidence shows that prevention, treatment, and harm reduction are necessary to save lives and protect our communities, but services for people who use drugs lack resources and political support.
The 2024 European elections must bring a paradigm shift. This manifesto lays down a vision for a pragmatic, innovative, and human rights-centred European drug policy that will deliver healthier and safer communities. We invite all European civil society organizations, parties, and candidates to endorse the following calls to action.
Together, we will build a drug policy that prepares Europe for the future.
#FutureDrugPolicyEU24
Open To Everyone, Initiated by Correlation – European Harm Reduction Network, NEWNet Enjoying Safer Nightlife.
SIGN AND DOWNLOAD THE MANIFESTO
Also in 🇫🇷, 🇨🇿, 🇮🇹, 🇪🇸, 🇩🇪, 🇭🇺, 🇷🇴, 🇱🇹, 🇪🇪, 🇲🇪.
The Principle of the Drug Policy Manifesto:

Ramp up investment in health and social care
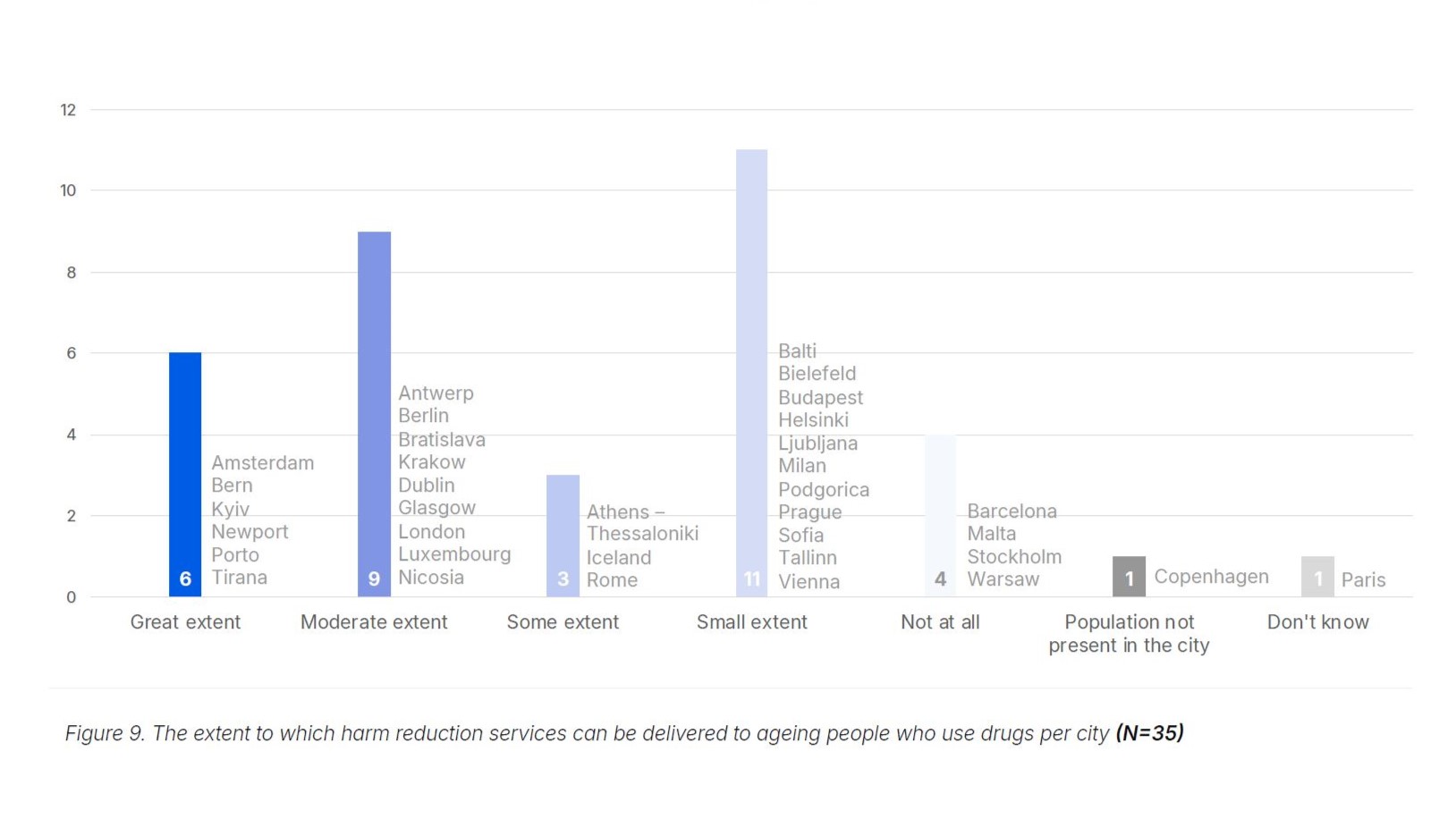
Drug use in Europe is at record levels, and the growing presence of new psychoactive substances, including synthetic opioids, has raised the alarm. Law enforcement and drug control will not stop this new threat, just as they have failed in other regions of the world. To be prepared for the future, the EU institutions must prioritise support and funding for integrated health and care services that are proven to work. A focus on services that support, rather than punish, people who use drugs is necessary to save lives and keep communities safe.
EU drug policy must be rebalanced, ending the current prioritisation of law enforcement over health. The EU institutions must ramp up investment and support for selective and indicated prevention programmes, evidence-informed voluntary treatment, life-saving harm reduction (including HIV/AIDS and HCV prevention, opioid assisted treatment, take-home naloxone, drug checking services, and drug consumption rooms), and community-based and community-led services that can reach out to everyone in need.

Abandon war-on-drugs policies
It is time to abandon war-on-drugs policies that, despite costing billions, have failed to reduce the size of illegal drug markets, to curb the power of organised crime or to reduce violence. Policies and narratives that stigmatise and blame people who use drugs and marginalised communities must be replaced with interventions grounded in evidence, inclusion, and human rights.
To ensure an integrated, holistic, and intersectional approach to drugs, EU health bodies must have a pivotal role in shaping EU drug policy. Drug policy must be mainstreamed across social, health and economic policies, and not be left at the hands of law enforcement alone.
The EU institutions must mainstream an inclusive, human rights and gender-based approach to drugs, including an unequivocal support for the decriminalisation of people who use drugs as a measure to remove stigma and improve access to services.
The new EU Drugs Agency must create indicators that monitor the effectiveness and impact of current drug policy approaches such as crime prevention and demand and harm reduction, including on stigma, access to services, and human rights, and conduct more policy-oriented research. EU bodies mandated to uphold human rights, EU values and the rule of law must also be involved.

Ensure civil society and community participation
A safer and more effective drug policy requires the involvement of civil society organizations that work every day with communities, can reach out to vulnerable populations, and are best informed of new trends in drug markets. EU drug policy must reflect the principle ‘nothing about us without us’, involving first and foremost affected communities and people who use drugs.
Mechanisms for civil society participation in EU drug policy, including the Civil Society Forum on Drugs in the EU, should be appropriately funded, supported, and meaningfully consulted by the European Commission, the EU Drugs Agency, and all relevant EU institutions. They should include representatives of affected communities, including people who use drugs, young people, women, and those disproportionately affected by criminalisation, stigma, and discrimination.
Explore innovative approaches, including responsible regulation
A pragmatic drug policy requires exploring innovative approaches to drug markets, including the responsible regulation of drugs such as cannabis, as a key measure to protect the health and human rights of communities, and reduce the power of organized crime. The EU should facilitate these innovations, and monitor their impact on health, safety, and human rights.
European policy makers must ensure that European laws and policies facilitate the adoption of innovative approaches to drug markets, including responsible regulation. The EU Drugs Agency should monitor the impact of drug policies and regulation, to allow for evidence-informed policy making. This will support mutual learning, increase uptake of best practices, contribute to pragmatic solutions, and prepare Europe for the future.

Already signed by…
Politicians & Decision-Makers
BELGIUM:
Bart Staes (MEP, Flemish Greens – Groen)
Saskia Bricmont (MEP, Ecolo / Greens/EFA)
Estelle Ceulemans (MEP candidate, PS – Parti Socialiste)
Matthieu Liessens (MEP candidate, PS – Parti Socialiste)
Yvan Verougstraete (MEP candidate, Les Engagés)
FINLAND:
Merja Kyllonen (MEP, Left Alliance)
FRANCE:
Alexandre Feltz (Deputy Mayor, Strasbourg)
Dominique Broc (Member of the Mairie de Chenevelles City Council)
GERMANY:
Kirsten Kappert-Gonther (Member of national parliament, Bündnis 90/Die Grünen)
IRELAND:
Luke Ming Flanagan (MEP, The Left group in the European Parliament)
Graham de Barra (MEP Candidate, Independent)
ITALY:
Massimiliano Smeriglio (MEP, Alleanza Verdi e Sinistra)
Luca Boccoli (MEP candidate, Alleanza Verdi e Sinistra)
Giuditta Pini (MEP candidate, Partito Democratico)
Andrea John Dejanaz (MEP candidate, Alleanza Verdi e Sinistra)
Luca Fella Trapanese (Councillor for Social Policies, City of Naples, Italy)
Jacopo Rosatelli (Councillor for Health and Social Affairs, City of Turin, Italy)
Paolo Ticozzi (Member of the Venice City Council / Partito Democratico, Italy)
LUXEMBOURG:
Clement Sven (Member of National Parliament, Luxembourg)
Daniel Silva (MEP candidate, Volt Luxembourg)
Philippe Schannes (MEP candidate, Volt Luxembourg)
Conny Jaroni (MEP candidate, Greens/EFA & Volt Europa)
MALTA:
Sandra Gauci (MEP candidate, ADPD Green Party, Malta)
Civil Society Organisations:
Almost 300 CSOs from the following countries have signed the Manifesto.
AUSTRIA:
Koje | taktisch klug
Students for Sensible Drug Policy International
InnovaDrug
Suchthilfe Wien
BELGIUM:
Modus Vivendi
European AIDS Treatment Group
Ex Aequo
Projet Lama centre psycho-médico-social
VAD
ARAS Romanian Association Against AIDS
Médecins du Monde Belgium - Dokters van de Wereld
Smart on Drugs
Free Clinic vzw
Odas Coordination
ASBL SOLAIX
ESPAS
CGG Noord-West-Vlaanderen
CAW de Kempen de Lange Gaank
Fedito wallonne
Gig (Health Promotion in Injecting Drug Use)
BOSNIA AND HERZEGOVINA:
The Chronic Viral Hepatitis Patients Association - B18
BRAZIL:
Rede Brasileira De Redução de Danos e Direitos Humanos
Plataforma Brasileira de Política de Drogas
BULGARIA:
Dose of Love Association
CANADA:
CAPUD - Canadian Network of People Who Use Drugs
Association des intervenants en dépendance du Québec
CATALUNYA:
Episteme. Investigació i Intervenció Social
Associacio Canaan-Pla De L'Estany
CROATIA:
Alternation Association
Life Quality Improvement Organisation FLIGHT
CZECHIA:
Asociace poskytovatelů adiktologických služeb, z.s.
SANANIM z.ú.
PREVENT 99, z.ú.
Kolpingovo dílo České republiky z.s.
Prostor plus, o.p.s.
Centrum sociálních služeb Praha
Association Of Social Care Providers Of Czechia
KOTEC o. p. s.
Středisko křesťanské pomoci Plzeň
Společnost Podané ruce, o.p.s.
Institut for Rational Addiction Policy (IRAP)
ANA, z.ú.
P-centrum, spolek
Kontaktní centrum - víceúčelová drogová služba
Darmoděj z.ú.
Unie LZZ
Zařízení sociální intervence Kladno
CYPRUS:
RESET - Research and Education in Social Empowerment and Transformation
DENMARK:
HealthTeam for the Homeless and Health in Front
Brugernes Akademi
ESTONIA:
Estonian Association of People Using Psychotropic Substances "LUNEST"
Lunest
MTÜ Ööhaldjad
FINLAND:
Finnish Institute for Health and Welfare
Humaania päihdepolitiikkaa ry
FRANCE:
Global commission on drug policy
RdR:RefletsduReel - Asud auto-support usagers de drogues
Fédération Addiction
AIDES
Association GrEID
Association Bus 31/32
ENCOD
ASUD
Sovape
NORML France
Forum Drugs Mediterranean-FAAAT
Techno Plus
CAARUD Lou Passagin
AEP
APSA 30
RdR:RefletsduReel
CSAPA BLANNAVES
Underground
FEDERATION ADDICTION
Association ITHAQUE
CSAPA BLANNAVES
Csapa OPPELIA
Sara Logisol
Nautilus RdR
Techno+
ithaque
Littoral Prévention Initiatives
Act Up Sud-Ouest
Nautilus
Freeparty
Addiction
Keep Smiling
CSAPA Soléa
Psychonaut
PlaySafe Paris, Paris LGBT
Culture Drogues
Psychonaut.fr
Afder.org & Old Timers Recovery un homme
Drogues et Société
L'Amicale RDR
Nouvelle Aube
Groupement Addiction Franche Comté
Health Without Barriers
Collectif Ensemble Limitons les Risques
Les Insoumis
Fédération addiction
SIDA Paroles 78
SOS Addictions
GEORGIA:
Eurasian Movement for the Right to Health in Prisons
GERMANY:
#MyBrainMyChoice Initiative
Fixpunkt e. V.
Akzept e.V. - Bundesverband für akzeptierende Drogenarbeit und humane Drogenpolitik
Basis - Beratung, Arbeit, Jugend und Kultur e.V.
Jugend und Kulturverein Halle e.V.
SONICS e.V.
Drug Scouts
Chill out e.V.
VIVID e.V.
Akzept e.V.
Audshilfe Dortund e. v.
Palette gGmbH
Integrative Drogenhilfe e.V.
Paritätischer Landesverband Hessen
IDH
BASIS-Projekt, basis&woge e.V.
Integrative Drogenhilfe e.V
Verein für Integration und Suchthilfe e.V.
Deutsche Aidshilfe
Aids Hilfe Frankfurt
GREECE:
Steps Non-Profit
PRAKSIS
Steps
PeerNUPS
Positive Voice
Self-organizing Initiatives for People who Use Drugs
HUNGARY:
Rights Reporter Foundation
INDIT Közalapítvány Bulisegély Szolgálat
Daath.hu - Hungarian Psychedelic Community
ELTE PPK; Behavioural Research Social Sciences and Services Ltd
Dát 2 Psy Help
Blue Point Drug Outpatient Centre
INDONESIA:
GAMMA Indonesia
ICELAND:
Matthildur, harm reduction organization
IRELAND:
Citywide Drugs Crisis Campaign
Ana Liffey Drug Project
Help Not Harm
Citywide Drugs Crisis Campaign
Rialto Community Drug Team
UISCE
Walkinstown Greenhills Resource Centre
Daish Project
Ballyfermot Advance Project CLG
Addiction Response Crumlin
Youth Workers Against Prohibition
RADE CLG
Kilbarrack Coast Community Programme
SURIA/Euronpud
ITALY:
LILA - Italyn League for Fighting AIDS
Forum Prävention - streetlife.bz
L' Isola di Arran
Forum Droghe
Parsec NGO
Lab57 - Alchemica, Bologna
NADIR ETS
LILA Onlus - Lega Italyna per la Lotta contro l'AIDS
L'isola di Arran ODV
Itanpud
ITANPUD APS
Itanpud
Itanpud
Chemical Sisters
Antigone onlus
CNCA - Coordinamento Nazionale Comunità di Accoglienza
ARCI
CGIL
ITARdD Itałian Harm Reduction Network
Gesco consorzio di cooperative sociali
la Società della Ragione
Substantia
LITHUANIA:
Eurasian harm reduction association (EHRA)
Support foundation "RIGRA"
Association of HIV affected women and their families
Support foundation "RIGRA"
Young Wave
NGO "Gilės sodas"
Coalition "I Can Live"
LUXEMBOURG:
4motion asbl. / PIPAPO
MALTA:
Harm Reduction Malta
Releaf Malta
MONTENEGRO:
NGO Juventas
Crnogorska mreža za smanjenje štete LINK / Montenegrin Harm Reduction Network LINK
NETHERLANDS:
Belangenvereniging Druggebruikers MDHG
Mainline
Legalize NL
LEAP NL
De Regenboog Groep
VOC (Union for the abolition of cannabis prohibition)
Harm Reduction Network/Trimbos Institute
NORWAY:
Association for Humane Drug Policy
Safer Youth
proLAR Nett
The Norwegian Association for Humane Drug Policy
POLAND:
PREKURSOR Foundation for Social Policy
Youth Organisations for Drug Action
PORTUGAL:
Médicos do Mundo
CASO
Kosmicare
MANAS/ GAT Portugal/ EuroNPUD
Associação Existências
Associação "Ninguém Pode Ficar Para Trás"- Porto Solidário 20
Acompanha, CRL
REPUBLIC OF MOLDOVA:
PULS COMUNITAR
ROMANIA:
ARAS - Romanian Association Against AIDS
Romanian Harm Reduction Network
Fundatia PARADA
Sens Pozitiv Association
ALIAT
SCOTLAND:
Scottish Drugs Forum
Crew 2000 Scotland
SERBIA:
Drug Policy Network South East Europe
NGO Re Generation
SLOVAKIA:
Odyseus
SLOVENIA:
Društvo SVIT Koper
Association SKUC
Društvo AREAL
Association DrogArt
Zveza NVO na področju drog in zasvojenosti
Association For Harm Reduction Stigma
SPAIN:
Governance Research Center - University of Salamanca
Asociación Stop SIDA
Metzineres SCCL
Kykeon Analytics
UNAD
Grupo de Trabajo sobre Tratamientos del VIH (gTt-VIH)
ICEERS - International Center for Ethnobotanical Education, Research and Service
Sociedad Clínica de Endocannabinología (SCE)
ARAIS
Asociación Amaina
Asociación Proyecto Hogar
Colectivo De Prevención E Incorporación CEPA
Asocación Progestión
ALAT
Federación Andaluza ENLACE
Asociación Punto OMega
Asociaciación Bienestar y Desarrollo
Asociación para la Prevención y Estudio de las Adicciones (APRET)
Fundacion Erguete-Integracion
Asociación Noesso
Asociación Bidesari
Fundación Ambit Prevencio
Asociación DESAL
Kykeon Analytics
SWEDEN:
Safe Haven Sweden
SWITZERLAND:
Groupement Romand d'Études des Addictions, GREA
Infodrog
ARUD Suchtzentrum
UKRAINE:
Alliance For Public Health (Drugstore Project)
ГОЗахідний Ресурсний центр Волна-Захід / Western Resource Center of All-Ukrainian Association of People with Drug Addiction
VOLNa всеукраїнське об'єднання людей з наркозалежністю / Charity Organization "All-Ukrainian Association of People with Drug Addiction (VOLNA)"
Charitable Foundation "Second Life"
UNITED KINGDOM:
ReShape/International HIV Partnerships
Asociación Punto OMega
Psycare UK
Benzo Research Project
Newcastle University
PostScript360
WALES:
Barod
EUROPE/GLOBAL:
EuroNPUD
Coalition PLUS
Youth RISE
European Sex Workers' Rights Alliance (ESWA)
D2 INNOLAB- Global Innovation Lab on Drug Policy & Sustainable Development - Global
AUSTRALIA:
AIVL
ECUADOR:
Anandamind
Parametria
FRENCH GUYANA:
Association guyanaise de réduction des risques (AGRRR)
NEPAL:
Recovering Nepal
SENEGAL:
Alliance Nationale des Communauté pour la Santé (ANCS)